The global health landscape is undergoing a profound transformation, driven by the relentless advancement of artificial intelligence. From remote rural clinics to sprawling metropolitan research centers, AI technologies are weaving themselves into the very fabric of healthcare delivery, promising a future that is more predictive, personalized, and accessible.
This is not merely an incremental improvement; it is a fundamental shift in how we understand, diagnose, and treat disease on a planetary scale. The potential to address long-standing inequities and leapfrog over traditional infrastructural limitations has never been more tangible.
At the diagnostic frontier, the impact of machine learning algorithms is nothing short of revolutionary. Consider the challenge of interpreting medical imagery. Radiologists and pathologists, the cornerstones of diagnostic medicine, are often burdened with immense workloads, leading to fatigue and the inevitable risk of human error. AI models, trained on millions of annotated images—X-rays, MRI scans, retinal photographs, and histopathology slides—are now achieving, and in some cases surpassing, expert-level accuracy in detecting conditions like cancerous tumors, diabetic retinopathy, and tuberculosis. These systems do not tire. They can work around the clock, providing a consistent second opinion and flagging subtle anomalies that might escape the human eye. This is not about replacing clinicians but about augmenting their capabilities, freeing them to focus on complex cases and patient interaction. In regions with a critical shortage of specialists, AI-powered diagnostic tools on mobile platforms can be a lifeline, enabling community health workers to perform sophisticated screenings and refer patients appropriately.
Beyond diagnostics, the power of AI to sift through immense datasets is unlocking new possibilities in drug discovery and development. The traditional process of bringing a new drug to market is notoriously slow, expensive, and fraught with failure. AI is poised to disrupt this paradigm. By analyzing complex biological data, including genomic sequences, protein structures, and vast repositories of scientific literature, AI can identify novel drug targets, predict how molecules will interact with the human body, and even design new candidate drugs from scratch. This significantly accelerates the initial research and pre-clinical phases. Furthermore, AI can optimize clinical trial design by identifying suitable patient populations and predicting potential adverse effects, thereby increasing the efficiency and success rate of these crucial studies. The result could be a faster pipeline for life-saving therapies, potentially reducing costs and getting treatments to patients in need much sooner.
Perhaps one of the most significant opportunities lies in the realm of public health and epidemic preparedness. The recent COVID-19 pandemic laid bare the vulnerabilities of global health systems. AI offers a powerful toolkit for a more proactive defense. By analyzing real-time data from diverse sources—news reports, flight patterns, satellite imagery, and anonymized mobility data—AI-driven models can provide early warnings of potential disease outbreaks, allowing health authorities to mobilize resources and contain threats before they spiral into pandemics. These systems can also model the potential spread of a pathogen, helping to guide public health interventions like social distancing measures and targeted vaccination campaigns. On a broader scale, AI can analyze population-level health data to identify trends in non-communicable diseases, such as diabetes and heart disease, enabling more effective and targeted prevention strategies.
The promise of AI extends directly to the point of care, personalizing the patient journey in unprecedented ways. Virtual health assistants and chatbots, powered by natural language processing, can provide 24/7 triage, answer basic health questions, and offer medication reminders, reducing the burden on primary care facilities. For patients with chronic conditions, AI can analyze data from wearable devices—tracking heart rate, physical activity, and sleep patterns—to provide personalized insights and early warnings of health deterioration, facilitating timely interventions. This shift towards continuous, data-driven health management moves us away from a reactive model of care to a proactive and preventive one, empowering individuals to take a more active role in their own well-being.
However, the integration of AI into global health is not without its profound challenges. The issue of data bias looms large. If AI models are trained predominantly on health data from wealthy, Western populations, they will perform poorly when applied to genetically diverse or underserved communities, potentially exacerbating existing health disparities. Ensuring representative and equitable data collection is paramount. Data privacy and security are also critical concerns. Health data is intensely personal, and robust frameworks must be established to protect this information from misuse and breaches. Furthermore, there is the risk of widening the digital divide. The benefits of AI could disproportionately accrue to high-income countries and privileged populations, leaving behind those in low-resource settings who lack the necessary digital infrastructure, electricity, and technical expertise.
To harness the full potential of AI for global health, a concerted, multi-stakeholder effort is required. Governments and international bodies must establish clear regulatory guidelines and ethical frameworks to ensure the safe, effective, and equitable deployment of AI technologies. This includes creating standards for algorithm transparency and accountability. Investment is urgently needed to build digital capacity in low- and middle-income countries, ensuring they are not merely recipients but active participants and co-creators in the AI health revolution. Crucially, trust and collaboration between technologists, healthcare providers, policymakers, and local communities must be fostered. AI should be developed with a deep understanding of local contexts and needs, designed to augment, not replace, the irreplaceable human element of care.
The journey of integrating artificial intelligence into the world's health systems is just beginning. The road ahead is complex, filled with both extraordinary promise and significant ethical hurdles. Yet, the vision is clear: a future where AI acts as a powerful ally to health workers, a sentinel for public health threats, and a catalyst for personalized medicine that reaches every corner of the globe. By navigating the challenges with wisdom, foresight, and an unwavering commitment to equity, we can steer this technological revolution toward its most noble goal: achieving better health for all of humanity.
In the sterile corridors of hospitals and the quiet desperation of homes, a silent battle is being waged. It's a fight for the most fundamental human need: breath.
Across the globe, patients with chronic respiratory conditions are raising their voices, demanding what many take for granted—reliable access to medical oxygen. Their stories form a tapestry of struggle, resilience, and an urgent call for systemic reform that can no longer be ignored.
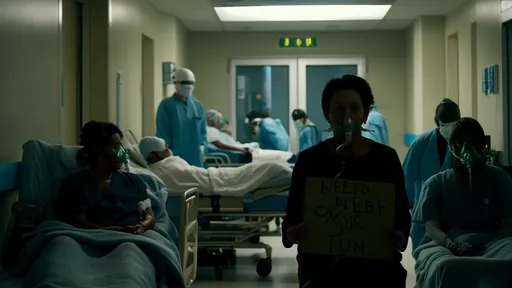
The COVID-19 pandemic brought the critical importance of medical oxygen into sharp, terrifying focus. Hospitals in wealthy nations scrambled to secure supplies as ICUs filled with patients struggling to breathe. But in low and middle-income countries, the situation reached catastrophic proportions. Images of people carrying empty oxygen cylinders through crowded streets became symbols of a broken system. What the world witnessed during those crisis years was not a new problem, but rather the dramatic exposure of a long-standing failure in global healthcare infrastructure. The pandemic merely pulled back the curtain on an issue that patients with conditions like COPD, pulmonary fibrosis, and severe asthma have faced for decades.
Behind the statistics are human beings whose daily lives are measured in breaths. Maria Gonzalez, a 68-year-old grandmother from Lima, describes her reality with stark clarity. "Every morning, I calculate how many steps I can take from my bed to the kitchen," she explains through a translator. "Not because my legs are weak, but because each movement costs me oxygen. I have to choose between making breakfast or having enough energy to speak with my grandchildren later." Maria suffers from chronic obstructive pulmonary disease, a condition that has progressively damaged her lungs over fifteen years. Her government-provided oxygen concentrator broke six months ago, and the replacement process has been trapped in bureaucratic limbo ever since.
In rural India, Sunil Patel navigates a different set of challenges. The nearest medical oxygen refill station is thirty kilometers from his village, a journey that becomes nearly impossible during monsoon season when roads wash out. His family has learned to ration oxygen, turning the flow rate down to minimal levels even when his oxygen saturation drops dangerously low. "We know it's not the right way," his daughter confesses, "but when the choice is between having some oxygen tomorrow or none at all, you learn to make compromises with safety." These compromises have consequences—Sunil has been hospitalized three times this year for complications that doctors say could have been prevented with consistent, adequate oxygen therapy.
The technological solutions for oxygen production and delivery are not particularly complex or new. Pressure Swing Adsorption plants can generate medical-grade oxygen from ambient air, concentrators can purify oxygen for individual use, and cylinders can transport oxygen to remote areas. The barriers are not scientific but systemic—a tangled web of economic, logistical, and political failures that have persisted for generations. In many developing nations, oxygen production remains centralized in urban areas, creating distribution nightmares for rural populations. Maintenance networks for medical equipment are sparse or nonexistent, meaning that a single broken part can render an entire oxygen system useless for months.
Economic disparities create what advocates call "oxygen apartheid." In wealthy nations, medical oxygen is considered essential infrastructure, as fundamental as electricity or clean water. But in poorer countries, it often becomes an out-of-pocket expense that pushes families into poverty. A study conducted across twelve African nations found that families of COVID-19 patients spent an average of fifty-five percent of their monthly household income on oxygen alone. When oxygen becomes a luxury commodity, the very architecture of healthcare equity collapses.
The human cost of these failures is measured in preventable deaths and diminished lives. The World Health Organization estimates that pneumonia alone kills over 800,000 children annually, with oxygen deprivation contributing significantly to these mortality rates. For every death, countless more patients experience permanent organ damage from prolonged oxygen deprivation or live with severely restricted quality of life. These are not abstract statistics but collections of individual tragedies—the father who can no longer work, the child who cannot play, the grandmother who misses family gatherings because she cannot travel without oxygen support.
Patient advocacy groups are emerging as powerful forces for change, transforming personal suffering into collective action. Organizations like the COPD Foundation and local grassroots movements are documenting patient experiences, lobbying governments, and creating peer support networks. Their demands are specific and actionable: integrate oxygen systems into primary healthcare, train community health workers in oxygen therapy, establish maintenance protocols for equipment, and regulate pricing to prevent exploitation. In Kenya, a coalition of patient groups successfully pressured the government to include medical oxygen in the national essential medicines list, a crucial first step toward making it accessible to all who need it.
Technology innovators are responding with solutions designed for challenging environments. Startups are developing solar-powered oxygen concentrators that can function during frequent power outages. Engineers are creating robust, easy-to-maintain equipment that can withstand dust, humidity, and rough transportation. Mobile applications now help patients locate oxygen suppliers, track their usage, and connect with healthcare providers. These innovations hold promise, but advocates caution that technology alone cannot solve what is fundamentally a political and moral problem.
The global health community is beginning to acknowledge oxygen as a specific priority rather than a peripheral concern. The WHO's Technical Specifications for Oxygen Concentrators and the establishment of the Global Oxygen Alliance represent important institutional steps. However, the transition from policy documents to functioning systems requires sustained funding, political will, and most importantly, continued pressure from those directly affected. As one advocate from Uganda put it: "They need to stop seeing oxygen as just another medical supply and start seeing it as a human right. You cannot have health without breath."
Perhaps the most profound shift occurring is in how patients themselves perceive their place in the healthcare ecosystem. Where once there was resignation, now there is growing insistence on participation in the decisions that affect their lives. Patients are no longer passive recipients of care but experts in their own conditions, valuable resources in designing systems that actually work for the people who depend on them. They understand the practical realities of oxygen therapy in ways that policymakers and even many healthcare providers cannot—the terror of watching the cylinder gauge approach empty, the calculation of whether to use oxygen for cooking or for sleeping, the shame of having to choose between breath and other basic necessities.
The battle for breath continues on multiple fronts—in government offices where budget allocations are decided, in communities where support networks are built, in homes where patients make daily calculations about their survival. The chorus of voices calling for oxygen reform grows louder each day, weaving together stories from every continent and economic circumstance. They remind us that the ability to breathe comfortably should not be a privilege determined by geography or wealth, but a fundamental dimension of human dignity. As this movement gains momentum, it challenges us to envision a world where no one must fight for breath, where oxygen is as reliably available as the air itself.

By Laura Wilson/Oct 13, 2025
By /Oct 14, 2025

By /Oct 14, 2025

By /Oct 14, 2025

By /Oct 14, 2025

By /Oct 13, 2025

By /Oct 14, 2025

By /Oct 14, 2025